



A child younger than 12 months has no control over their bladder and bowel movements. Between the ages of 12 and 18 months, they have little control, and by the age of 24 to 30 months, they start developing more control over their bowel and bladder by holding and release their urine and stool voluntarily.
Why do bladder and bowel incontinence happen?
A child’s typical bowel and bladder movement development might take longer than 30 months to appear due to some dysfunction in the muscles, sensory processing, respiratory system, or even diet.
According to Conway (2007), the term Bowel and Bladder Dysfunction (BBD) is used to describe the spectrum of lower urinary tract symptoms accompanying a bowel disturbance in the form of constipation and/or encopresis.
BBD* includes difficulties with regular bowel and bladder movements in children. As the bowel and the bladder share the same nerves and even some muscles, a full bowel can put extra pressure on the bladder and cause leakage, often leading children with constipation to also experience urinary incontinence.
What is the difference between incontinence and constipation?
Incontinence is the lack of voluntary control over urination or defecation. The cause of pediatric incontinence is often related to a lack of strength or coordination of the muscles that make up the pelvic floor.
Constipation occurs when bowel movements become less frequent and stool is difficult to pass. Your child may be constipated if they have less than three bowel movements in a week, or if their stool is large and hard or looks like “rabbit droppings”. The constipated child may be straining or experiencing pain or even bleeding during or after a bowel movement.
If your child is above the age of one, soiled pants can be another sign of constipation, as runny stool may leak out around the hard stool. This is called overflow soiling or encopresis.
Causes of Bowel and Bladder Dysfunction (BBD)
- Muscular:
- Pelvic floor dysfunction/weakness; or,
- Core weakness.
- Respiratory: Inefficient diaphragmatic breathing in coordination with the pelvic floor.
- Sensory processing:
- Tactile hyperactivity: some children dislike the sensation of pooping, wiping, or even sitting on a hard seat, so they hold the poo to avoid the sensation.
- Diet: Some foods irritate the bladder―including tomato-based products and carbonated drinks, among others―while others cause constipation, such as dairy, red meat, and fast and processed food. Also, a lack or excess of fiber plays a role.
- Congenital conditions that cause kidney, urethra, or intestine malformation.
- Medication for ADHD and anticholinergics.
What is the pelvic floor?
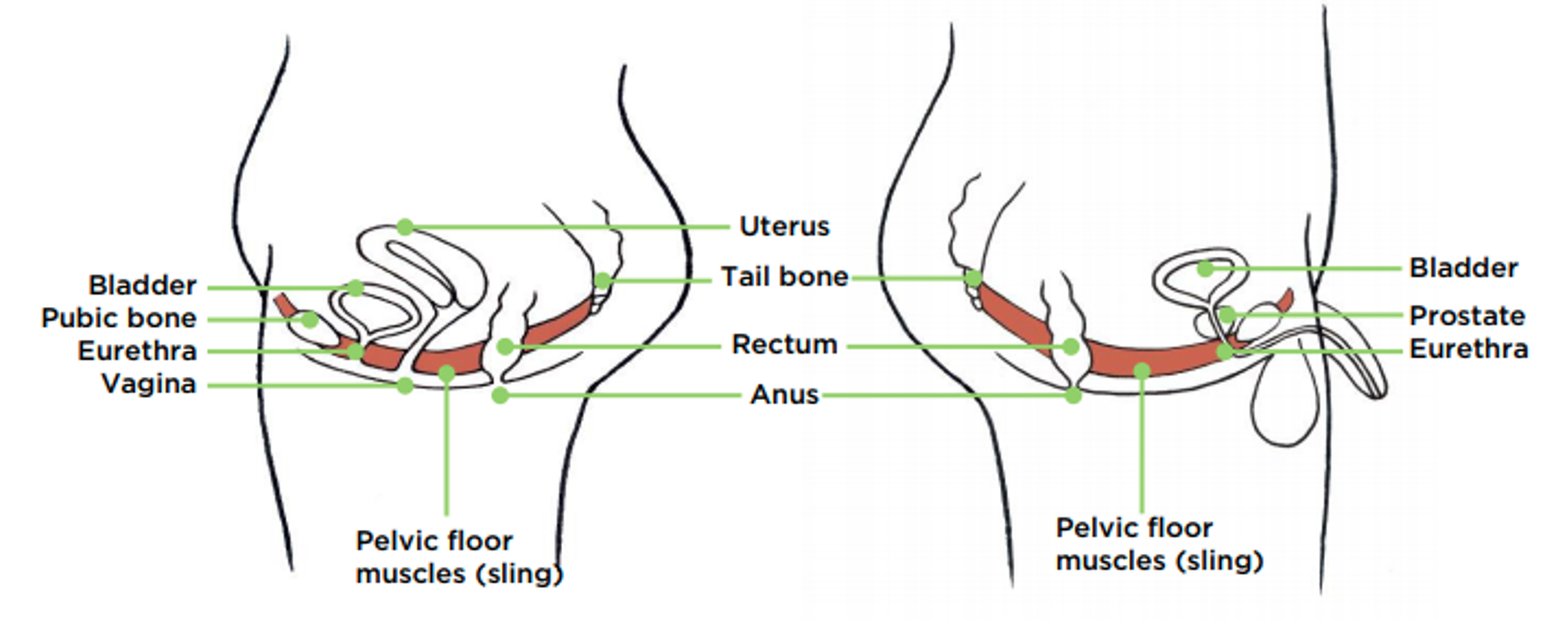
The pelvic floor comprises muscles and other tissues that form a structure extending from the pubic bone to the tailbone, as per the below illustrations. It supports the organs of the abdomen and pelvis, including the intestines and bladder, while helping control bladder and bowel activities.
Side view of pelvic floor muscles and the organs they support
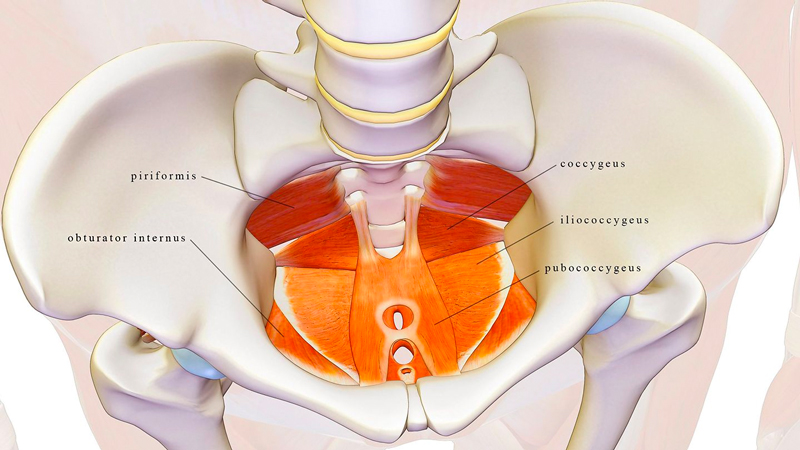
Internal view of pelvic muscles
Symptoms of Bowel and Bladder Dysfunction (BBD)
- Daytime wetting
- Bedwetting or enuresis, also called nighttime incontinence: a child older than 5 years involuntary urinates while sleeping. Pelvic floor training is an effective treatment for enuresis.
- Overactive bladder: causes a frequent and sudden urge to urinate, which may be difficult to control. The bladder signals to the brain that it is full and needs to be emptied, even though it is not entirely full. Your child may feel an urgency to urinate multiple times during the day and night, experiencing an unintentional loss of urine.
- Underactive bladder: bladder movements are less than three times in 24 hours or absent for around 12 hours.
- Voiding dysfunction: abnormally slow and/or incomplete emptying of the bladder.
- Constipation: having hard bowel movements and not having them often enough. Constipation that does not respond to standard therapy or lifestyle changes is called intractable constipation.
- Frequent leakage of urine or leaking of stool.
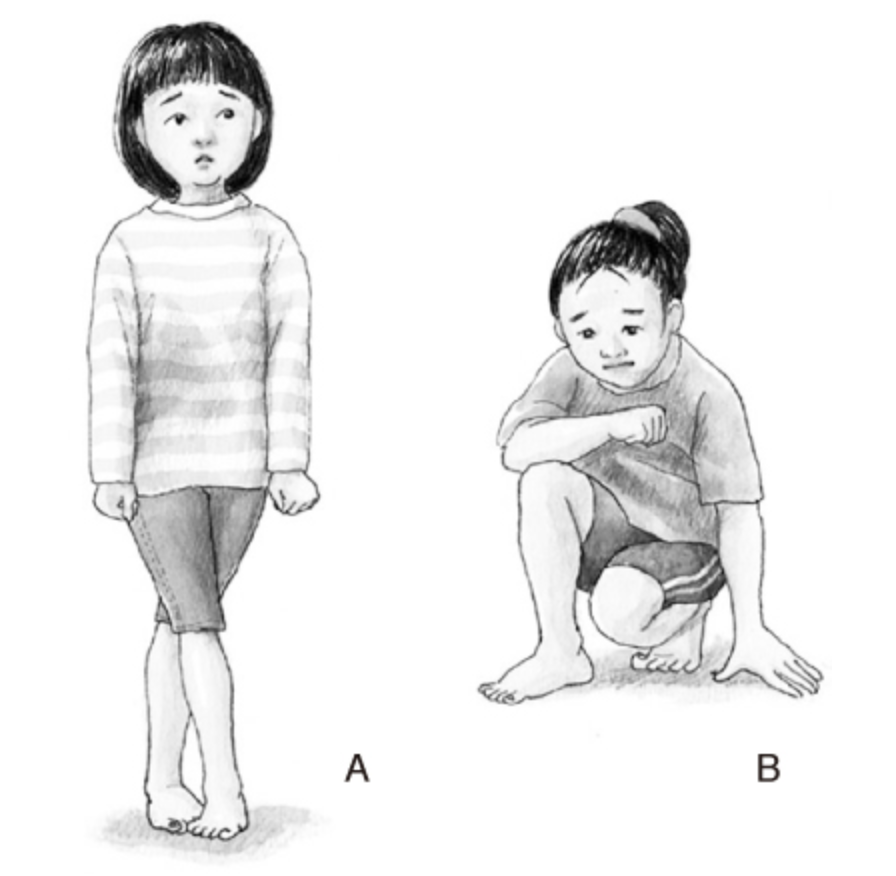
- Urine or stool holding maneuvers: the child does things to avoid going to the bathroom, such as squatting, leg crossing, holding the genital area, back arching, moving back and forth, straightening legs, tiptoeing, and standing stiff. Squatting is often a holding maneuver used by children when they need to urinate by placing their heels against the perineum. A variant involves energetically crossing the legs. These maneuvers are known colloquially as the “pee dance”.
High Hopes’ bowel and bladder rehabilitation program
At High Hopes Pediatric Therapy Center, our pelvic floor therapist offers a comprehensive program to help treat the most common bowel and bladder conditions, which includes:
- Structured assessments and standardized tests for potty training readiness, toilet habits related to tactile hyperactivity, bowel and bladder chart, core and low tonus, etc.
- Urotherapy: behaviors and diet strategies to improve toilet habits.
- Soft tissue techniques to relieve constipation.
- Core and pelvic floor strengthening exercises.
- Bladder training: a form of behavior therapy that treats urinary incontinence by increasing both the amount of time between emptying the bladder and the amount of urine the bladder can hold.
- Various diaphragmatic breathing techniques. The diaphragm and the pelvic floor have a pressure relationship: when you inhale, the diaphragm drops, increasing the space in the lungs and moving the abdominal organs forward, and the pelvic floor drops as well.
- Orientation regarding toilet seat posture and positioning to support pelvic floor muscle recruitment and relaxation.
- Sensory integration for children with sensory difficulties related to fecal retention (functional constipation).
- Toilet training: we can provide potty training to your child and can help them solve any identified challenges by, for instance, supporting them to recognize their body signals or to overcome sensory difficulties.

Early intervention is essential to avoid worsening gastrointestinal disorders and other complications, as mentioned by Morgan (2019), such as urinary tract infections (UTIs) or vesicoureteral reflux (an abnormal flow of urine from bladder to the tubes that connect your kidneys to your bladder), resulting in renal scarring and psychosocial problems.
Disclaimer: this article is for educational purposes only and is not intended to replace a medical evaluation.
BBD* Bowel and Bladder Dysfunction



