




In the initial months after birth, it’s not unusual for parents to seek consultation with their paediatrician or a physical therapist due to concerns of their infant exhibiting flattening of the head, a head tilt on one side, looking or even rolling in one direction. These are a few indicators that may suggest your child is experiencing a head deformity or tightness in the neck muscles.

The most common type of head deformity, referred to as Positional Plagiocephaly, denotes an asymmetrical flattening of the skull, often observed in typically developing and neuro diverse infants. Positional Plagiocephaly appears to manifest in the first few months of life and be age dependent. In 2023, the prevalence of healthy infants with head deformities accounted for 46.6% of 3-month-olds.

There has been a significant increase in the past 20 years of Plagiocephaly following the 1992 introduction of the “Back to sleep” campaign. It encouraged infants to sleep on their backs and sides, rather than front, to reduce the incidence of Sudden Infant Death Syndrome (SIDS). In addition, the increased access and commercialisation of containers such as bouncers, standers and walkers has resulted in babies getting less floor time and therefore less opportunities to learn to move and explore their surroundings.
The most common associated finding in infants with Positional Plagiocephaly is Torticollis. This term refers to the postural positioning that occurs when the head is twisted and turned to one side often because of muscle shortening. This tightness limits an infant’s ability to move their neck through full range of motion, thus contributing to the flat head shape.
How can they occur?
There are multiple reasons a head can become misshapen or torticollis develops, and it can occur prenatally or postnatally. However, these are some of the most common causes:
- Occurrence of a difficult labor leading to instrument-assisted delivery, such as ventouse or forceps.
- Fetal positioning in the womb, especially if the baby is larger in size or in a breech position.
- Presence of a pre-existing preference for head turning, such as from the baby’s favoured sleeping or feeding positions.
- Insufficient tummy time and limited variation in positions during awake periods.
- Premature birth, as babies born early often have softer skulls that are more susceptible to moulding.
- As a consequence of a birth acquired injury i.e. brachial plexus injury or spastic hemiplegia whereby a head turn preference develops from the offset due to underuse of the affected side.
How can physiotherapy help?
Positional head deformities and head turn preferences are a common cause for referral amongst paediatric physical therapists. Evidence states that if a head deformity is observed, then early physical therapy and education can prevent the progression of the deformity or torticollis developing ( APCP 2020). Reshaping of the head is most effective in the first 6 months when the skull is more pliable. In addition, as the baby learns to move and vary their position, the pressure on the flattened area of the skull is reduced.
There is a known link between infants with Plagiocephaly and developmental delay, largely gross motor in nature (Martinuik 2017). Therefore, a physical therapist will typically undertake a thorough developmental assessment alongside treating the deformity/preference. If the head turn preference has led to difficulties with function or positioning i.e. side-lying, rolling, bilateral hand use for play or sitting development, then the physical therapist will address these in the session.
In the case of head deformities, physical therapy often involves exercises to strengthen the neck muscles and improve head control. This can help correct the deformity and promote more symmetrical growth of the head.
Active movement and participation are proven to be most effective in managing head turn preferences, however in the instance of shortening in the neck muscles than gentle passive stretches, manual therapy techniques and positioning strategies can assist in improving range of motion and a neutral head position.
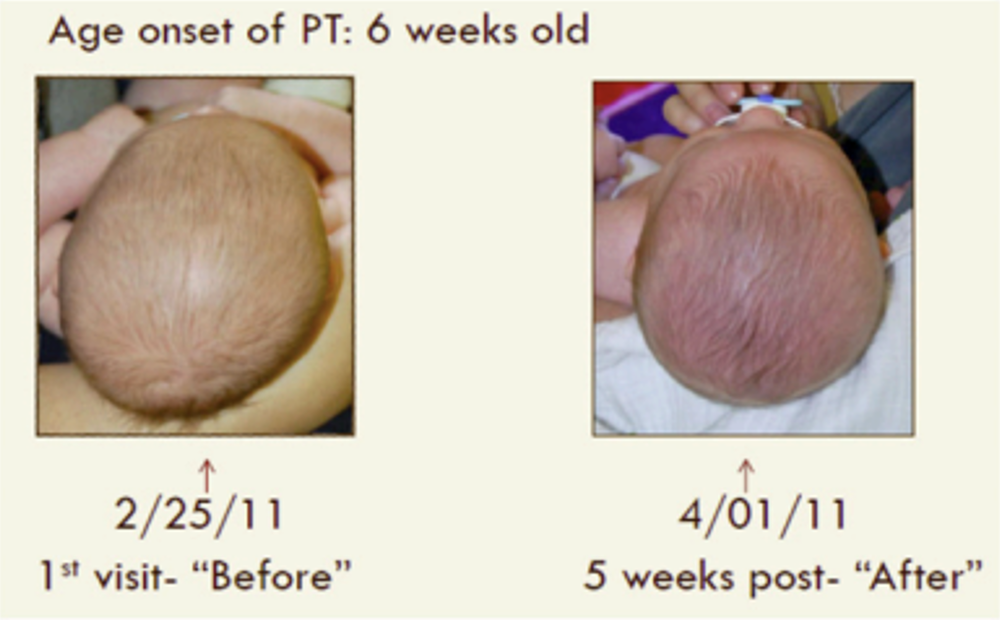
Here is an illustration of the treatment results following five weeks of physical therapy intervention as reported by Kuo A et al. 2014.
Physical therapists will work closely with the parents on education/counselling alongside other potential healthcare professionals such as paediatricians, orthopaedic surgeons or orthotists if a child is wearing a helmet. Evidence suggests that helmets are most effective in the correction of severe cases of positional Plagiocephaly, rather than mild or moderate cases (Wiyk 2014).
Signs your Infant may benefit from physical therapy:
- Mainly looking to one side when lying on back.
- A head tilt on one side.
- Flattening of the back of the head or one side.
- Difficulty holding head up beyond 3 months of age.
- Poor tolerance of tummy time.
- Rolling only in one direction.
- Tolerating side-lying only on one side.
- Using one arm less during reaching and grasping.
Tips for Parents:
Sleeping: Alternating the end of the cot the babies sleep in or even the position of the cot within the bedroom will encourage baby to face both directions as babies are often attracted to the light or sound source within a room.
After the baby has fallen asleep, repositioning their head to the non-preferred side can take the weight off the flattened area.

Playtime: Tummy time position is particularly important during awake time as it encourages the baby to develop head control, take weight through their arms and removes the pressure off the back of the skull.
Supported side-lying during play is another positional change and if the baby already has flattening, then a preference would be lying away from that side.
Limiting time in bouncers, strollers and car seats where there is uneven pressure on the head is also important.
Feeding: If baby is bottle fed, alternate the arm the baby is fed from, positioning the bottle in midline or slightly away from the preferred side.
If breastfed, then again alternating sides is optimal. In the instance of a baby having a head turn preference or restrictions in neck movements, then consider different feeding positions i.e. “rugby hold”. A physiotherapist or lactation consultant is able to explore this further with the parent.
Travel: Placing the babies non- preferred side closest to the window can stimulate more head turning. Due to the containment and more rigid material of a car seat, it is recommended that it is purely used for travelling and not outside the car due to the impact on the child’s head shape.

Holding/carrying: Positioning the infant close to the parent’s chest and turning their head to their non-preferred side can provide a gentle stretch whilst carrying.
In addition, facing the infant away from the parent in a side-lying position with their ear resting in the crook of the elbow can assist in limiting head turn to the preferred side and improve range of movement.
Overall, physical therapy is an essential part of treatment for children with head deformities and head turn preferences, particularly if home strategies or self-correction have proven to be ineffective. Not only can it improve a child’s physical function, but prevents any future limitations in meeting motor milestones or being able to access the environment.
At High Hopes, we support your child’s development from birth through to school age. If you have further enquiries about this condition, then kindly contact the centre for guidance and support.
Sources
- Paediatric Society of Neurosurgery, 2023., Epidemiology of Positional Plagiocephaly in Children.
- Van Wijk R, van Vlimmeren L, Groothuis-Oudshoorn C, Van der Ploeg C, IJzerman M, Boere-Boonekamp M. 2014., Helmet therapy in infants with positional skull deformation: randomised controlled trial. BMJ;348:g2741.
- Bialocerkowski A, Vladusic S, Choong W. Prevalence, risk factors, and natural history of positional plagiocephaly: a systematic review. 2008., Developmental Medicine and Child Neurology;50(8):577-86.
- Martiniuk A, Vujovich-Dunn C, Park M, Yu W, Lucas B. 2017., Plagiocephaly and Developmental Delay: A Systematic Review. Journal of Developmental & Behavioral Pediatrics;38(1):67-78.
- Association of Paediatric Charted Physiotherapists, 2020. Head turning preference and Plagiocephaly- information to parents and carers.
- De Bock et al, Arch Dis Child., 2017. June 102 (6) Deformations Plagiocephaly in normal infants: a systemic review of cause and hypotheses.
- Plagiocephaly and brachycephaly (flat head syndrome) – NHS (www.nhs.uk), 2022.
- Kuo, A, Trisavit, S, Graham, S., 2014.Congenital Muscular Torticollis and Positional Plagiocephaly. Paediatrics in Review, 35 (2).



