




Speech is the most complicated motor act that children will ever learn. They must practice controlling more than 100 muscles at once to move their jaw lips and tongue at the right time to get into the right place in order to produce even the shortest word. These muscles begin to work together between the ages of five and ten months old, when babies start to babble. Babbling then incorporates various sounds as it slowly begins to resemble conversational speech, especially in terms of rhythm, until babies start uttering the first work around twelve months of age.
As you may have already read in in High Hopes May, 2018 blog post “What do I do if my child is not talking?”1, when children are late to develop in any area, they are normally seen by a pediatrician. A General Practitioner is often the first professional to identify that there is a problem with a child’s language, communication or the way speech sounds are produced. “Speech sound disorder” (SSD) or “Speech Delay” are broad terms used to indicate that a child has trouble producing speech sounds.
There are several other labels for subsets of children who have a certain kind of speech sound disorders that are used by Speech and Language Therapists: Inconsistent Phonological Disorder, Phonological Delay, Dysarthria, Apraxia of Speech/Verbal Dyspraxia and Articulation Disorder. These labels indicate the primary behaviour that a child exhibits and allow the Speech Therapist to highlight and address the main challenge that the child is facing. Specific difficulties may be related to planning and programming speech movements, finding the right articulatory placement, discriminating or categorizing speech sounds. For example, “Childhood Apraxia of Speech” is a diagnosis for children who find planning and programming speech movements particularly challenging. More information on Apraxia and its treatment can be found in High Hopes March, 2018 blog post blog post2.
For some children, Speech Delay is a consequence of a known physical cause such as hearing loss, cleft lip/palate, ankyloglossia, apraxia and dysarthria. However, in most cases the causes are unknown. Young children who have frequent ear infections are at an increased risk for having speech sound disorders because of the temporary loss in hearing that they may experience[3].
When should I be concerned?
There are several ways to estimate approximately how well a child’s sound system is developing. There might be a mild difficulty in the production of only one or two sounds, or there may be so many errors causing the child’s speech to be not understandable. Most typically developing child’s speech should be understood by an unfamiliar listener by age five. However, children are not expected to be able to necessarily produce the most complex sounds, such as “s” or “r”, until around their eighth birthday 4.
There are, in fact, established ages when most children say a given sound correctly: mistakes should decrease as the child develops and as their intelligibility improves. If a child still cannot correctly produce a given sound after a certain age, a speech sound disorder may be present. There are several different types of speech sound errors: deletions (e.g., saying ‘nana for banana), additions, distortions and substitutions (e.g., saying Tate instead of Kate). Following an assessment, your Speech and Language therapist will explain why certain errors are developmentally appropriate and certain are not. For example, a substitution of /t/ for /s/ is not a concern at age 2 but it is at age 4. However, using a “th” sound instead of /s/ at age 5 (this phenomenon is commonly referred to as a “lisp”) may not be a concern at all, in some cases.
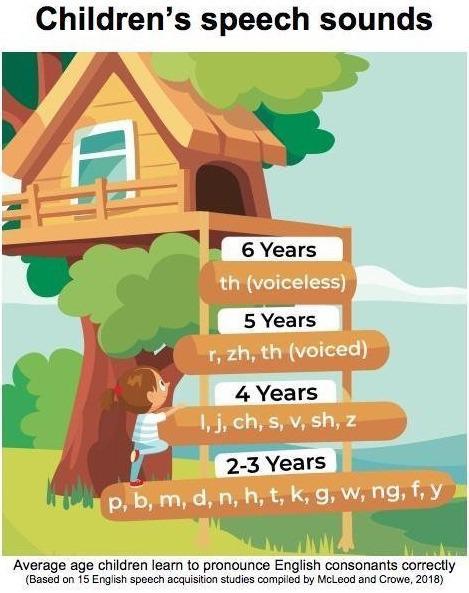
Please refer to the milestones illustrated in the picture below to get a sense of when a child is expected to produce the sounds of English correctly.
Children with Complex Needs and Speech Delay
You may already know that your child’s development is atypical and, in many instances, it may not be useful to compare your child’s performance to the norm or ask your child to go through a generic articulation test. At High Hopes, we are a team of skilled professionals who will attend to all your child’s needs. Every day, we cater to children who have significant attentional problems, severe speech sound disorders or are minimally verbal. We will minimize barriers to allow any child to access the best care possible, starting with a thorough assessment.
As highly qualified speech therapists, we know best practice is to keep things natural and functional to set the stage for your child’s success. For example, we may choose to evaluate strength and speed of oral movements through having a feeding specialist assist and observe your child at meal times. We will take note of the range of movement in the tongue while eating, jaw grading and range of motion while chewing as well as cheek and lip recruitment while swallowing. If your child is able to imitate our model, we may ask him to imitate our oral movements as we go through the Oral Motor section of the Nuffield Dyspraxia Programme (NDP3) or the Kauffman Praxis Test.
We are particularly proud to offer the Nuffield Dyspraxia Programme (NDP3), which is widely recognized by the scientific community as one of the most evidence-based approaches for the management of Childhood Apraxia of Speech/ Developmental Verbal Dyspraxia and Severe Speech Sound Disorders.
When treating children with Speech Sound Disorders, the Nuffield therapy approach aims “to build motor programs for speech in small graded steps, working from single sounds to complex words”5. The program is detailed, structured and systematic like no other but also allows for personalization and can be used in conjunction with other techniques/ approaches. For example, while working on sequencing long vowels and introducing diphthongs in new sequences by using the Articulograms6 and the Transition Worksheet from the NDP3, the clinician might choose to use PROMPT’s tactile cues to facilitate speech production, highlight timing and transitions or other aspects that are better addressed with tactile cueing6.
Because of the way the NDP3 is designed, it can be used both with younger and older children. The therapy material is appropriate for all ages and it includes thousands of therapy cards, illustrations, activities, games and worksheets that facilitate carry-over and generalization of skills at home by motivating children and the adults working with them to keep practicing. Our Apraxia team is trained in all the available approaches, including NDP3, PROMPT7, K-SLP8, DTTC9, ReST10, OPT11, and routinely joins forces with other specialists to help your child overcome any possible obstacle on the way to better speech.
If you want to know more
Feel free to email me at ebreglia@highhopesdubai.com if you want to know more about how we can help you to support your child’s development.
I am also happy to answer questions about:
- Speech sound development
- Ways to help children improve their speech production
- Expectations of Speech and Language Therapy input
- Expectations of specific Speech and Language Therapy approaches
Sources:
1 https://www.highhopesdubai.com/blog/what-do-I-do-if-my-child-is-not-talking.html
2 https://www.highhopesdubai.com/blog/what-is-apraxia.html
3 https://www.asha.org/public/speech/disorders/Speech-Sound-Disorders/
4 https://www.asha.org/public/speech/development/chart/
5 Nuffield Centre Dyspraxia Programme 3 (NDP3), Therapy Manual, Chapter 4, Introduction to the Nuffield therapy approach and treatment Planning, p. 73
see also: https://www.ndp3.org/treatment-approach/
6 Stephens, H.; Elton, M. (1986) Description and Systematic Use of Articulograms. College of Speech and Language Therapists Bulletin: December
7 https://www.promptinstitute.com/page/FamiliesWIP
8 http://www.kidspeech.com/kslp/
9 https://www.childapraxiatreatment.org/WhatIsCASandDTTC.aspx
10 http://sydney.edu.au/health-sciences/rest/families.shtml
11 https://talktools.com/pages/what-is-opt